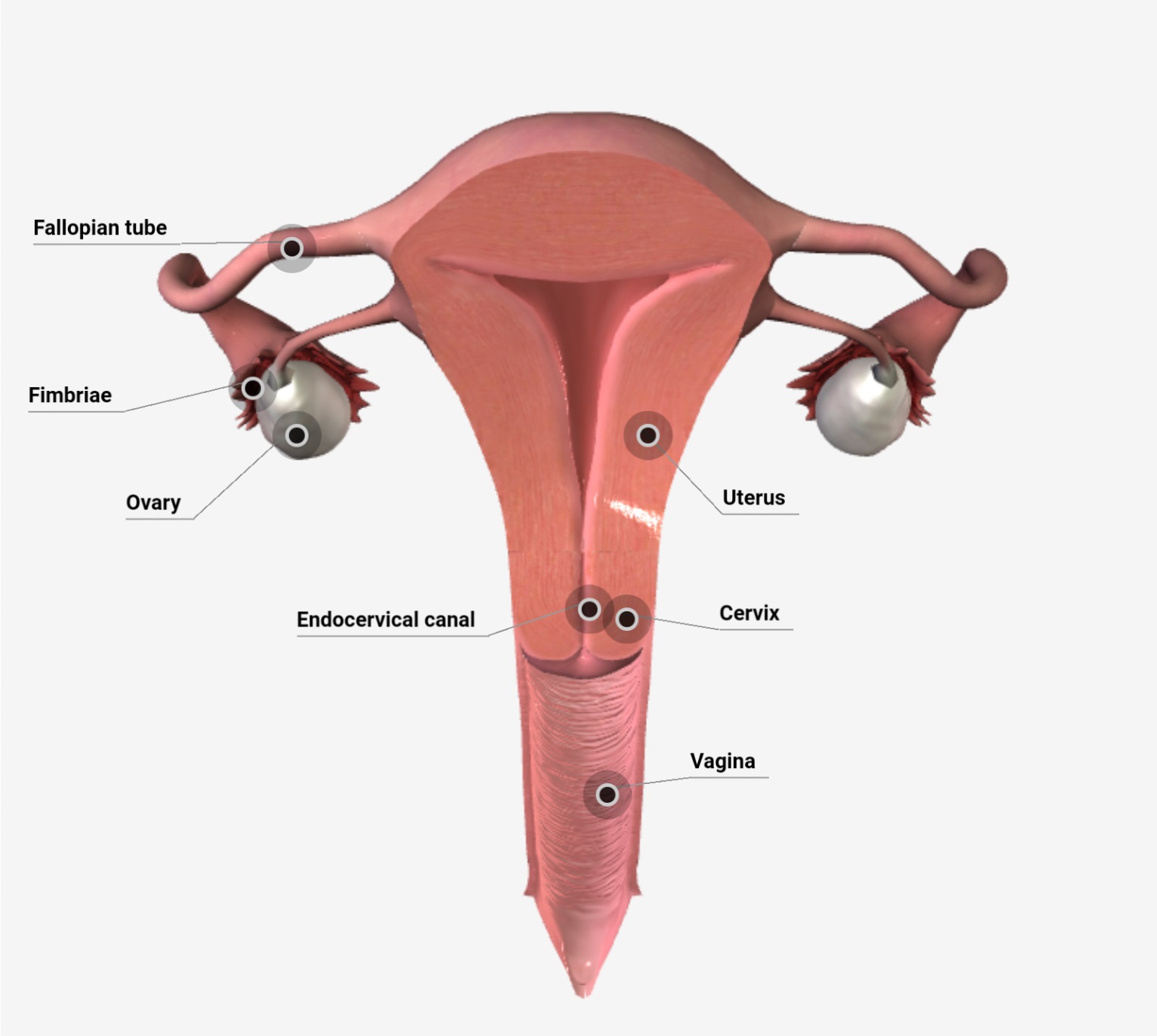
Both Benign and malignant tumours are common in the cervix. Cervix is the site of lesions that include cervical dysplasia and carcinoma in situ, cervical intraepithelial neoplasia (CIN), also termed as squamous intraepithelial lesions (SIL).
(A) CERVICAL POLYPS:–
-These are localized benign proliferations of endocervical mucosa though they may protrude through the external os.
Morphological features-
Grossly: Is a small (up to 5 cm in size) bright red, which is frequently pedunculated but may be sessile.
Microscopically: Most of the polyps are endocervical polyps which may show squamous metaplasia, the stroma of polyp is composed of fibrous tissue with inflammatory infiltrate with dilated mucus-secreting glands.
(B) SIL/CIN:-
– Dysplasia, CIN, carcinoma in situ, and SIL are synonymous.
Etiopathogenesis:-
(1)Women with cervical cancer have several risk factors:
- Early age of sexual activity.
- Multiple sexual partners.
- Persistent HIV infection.
- Potential role of high risk male sexual partner such as promiscuous male having multiple sexual partners.
(2) Women having persistent HIV infection or have another cofactor such as cigarette smoking or immunodeficiency.
(3) Circulating tumour specific antigens and antibodies to virus-specific antigens are identified on tumour cells.
(4) Ultrastructural studies of the cell revealed mitochondria and free ribosomes. On the basis of schiller’s test in which suspected cervix is painted with a solution of iodine and potassium iodide. The cancerous focus if present fail to stain because of the lack of glycogen in surface cells.
Morphological features-
-No feature of cellular atypia found in dysplasia or carcinoma in situ except that the changes begin at squamocolumnar junction.
Histologically- The distinction between various grades of CIN, general dysplastic cells distributed in the layer of squamous epithelium for varying thickness, accordingly graded as mild, moderate and severe dysplasia and carcinoma in situ.
- In mild dysplasia, abnormal cells extend up to 1/3 rd thickness from the basal to the surface layer.
- In moderate dysplasia, up to 2/3 rd.
- In severe dysplasia, these cells extend from 75 – 90% thickness of the epithelium.
- In carcinoma in situ, the entire thickness from the basement membrane to surface shows dysplastic cells.
-Atypical cells migrate to the surface layer from where they are shed off into vaginal secretions in a pap smear.
(C) INVASIVE CERVICAL CANCER: –
-In this 80% of epidermoid squamous cell carcinoma.
Morphological features–
Grossly- It may indicate 3 types of pattern, fungating, ulcerating and infiltrating.
-Fungating pattern appearing as cauliflower like growth. It arises from the squamocolumnar junction. Advance stage characterized by destruction and infiltration into an adjacent structure including urinary bladder, rectum, vagina and regional lymph node. And distance metastasis occurs in lungs liver, bone marrow and kidney.
Histologically-
- Epidermoid (squamous cell) carcinoma comprises 70% of that.
- Adenocarcinoma – comprise about 20-25% of cases. It may be well-differentiated mucus-secreting adenocarcinoma.
- Others remaining 5% as are a variety of other patterns.