Events & Clinical findings in the First stage of labour
In this stage preparation of the birth canal occurs to expel the fetus during the 2nd stage of labour. It is a Cervical stage that starts from the onset of true labour pain and ends with full dilatation of the cervix. Its duration is about 12 hours in primigravidae and 6 hours in multiparae.
The events in this stage are as below-
Dilatation of cervix
-Dilatation begins in the prelabour phase, because of the softening of the cervix, hypertrophy of the cervical mucosal membrane, increased vascularity, fluid accumulation between the collagen fibers, and break down of collagen fibrils by collagenase & elastase enzymes.
Uterine contraction & retraction- When the upper segment (fundus) contract & retract the lower segment (isthmus) & cervix dilate as the longitudinal muscle fibers of the upper segment are attached to the lower segment circular fibers like a bucket holding fashion, so with each contraction cervix become dilate, shortened & retract.
A force from behind (vis-a-tergo)- There is a downward push of the presenting part of the fetus & an upward pull of the cervix over the lower segment.
Fetal axis pressure-There is a mechanical stretching in the longitudinal lie, the fundal contraction (a contraction of circular muscle fiber in fundus) causes straightening of the fetal vertebral column, so the pressure is created by a fetal axis on a cervix hence it dilates but this is absent in transverse lie.
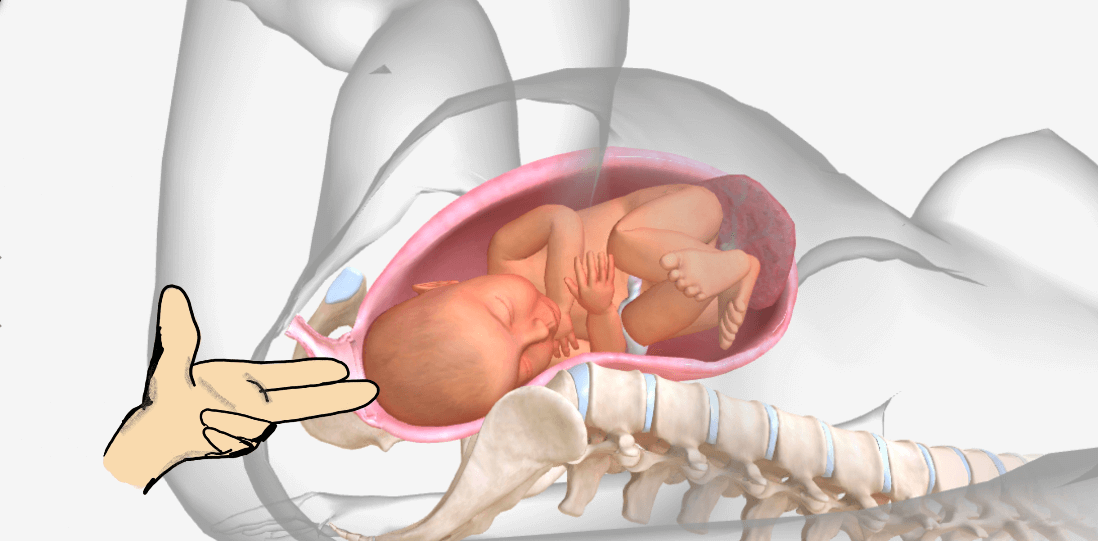
Bag of membrane-In vertex presentation the fetal head creates a girdle of contact as it sinks into pelvic brim & is well fit into the lower segment so the amniotic fluid (liquor) is divided into compartments, one above the girdle of contact with a good amount where the fetal body lies within it, is hindwaters & below the girdle is a scanty amount of liquor is forewaters. When uterine contraction occurs the pressure within the liquor increases so the loosely attach fetal membrane with the decidua become detach & enters into the cervical canal, the hydrostatic pressure within the forewaters then causes cervical dilatation.
Effacement of the cervix (Taking upward)-
The muscular fibers of the cervix are pulled upward to merge with the lower uterine segment with the thinning of the cervix. In multigravidae, effacement & dilatation occurs simultaneously, but in primigravidae effacement occurs prior to dilatation of the cervix. The expulsion of the show (blood-tinged cervical mucus plug) is caused by effacement.
Formation of the lower uterine segment-
There is no marking between the 2 segments of the uterus (upper & lower) but when the contraction begins the upper active segment is demarcated by lower passive segments, by a physiological retraction ring & there is progressively thickening of the upper segment with the thinning of the lower segment.
The clinical features in this stage are-
-The pain is felt with the uterine contraction, is passes off with relaxation in between the contraction. It is situated anterior to the abdomen with hardening of the uterus and comes at regular intervals of 3-5 min, lasting about 45 seconds in the late first stage.
-The progressive dilatation & effacement can be measured through the vaginal examination. Dilatation indicates the dilatation of external os & effacement means the thinning of the cervix into the vaginal wall. In primigravidae mother effacement occurs first, with a few dilatations, feeling like a paper, it measured by a fingering method but recorded in c.m. like 1,2,3, or fully dilated-10 c.m. On average 1 finger equals 1.6 c.m.
-Effacement measured through percentage -25%, 50%, 100%.
-The membrane remains intact (not ruptured) until full dilatation but it can rupture after the onset of true labour, but before full dilatation, it is termed early rupture. When membrane rupture before the onset of labour is a premature rupture.
-With the rupture of the membrane, a liquor escapes out through the vagina & thus increases uterine contraction.
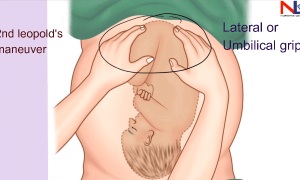
-In peak uterine contraction bulging intact membrane can be felt through vaginal examination & the membrane goes relax as contraction passes off, and comes in contact with the fetal head, the station, presentation, presenting part, denominator, the position could be assessed in relation to the maternal pelvis by the bimanual vaginal method.
-The mother becomes exhausted and fatigued, the pulse rate is increased by 10-15 beats/min. & blood pressure increases by 10mmHg during contractions & these values go to normal as contraction passes off.
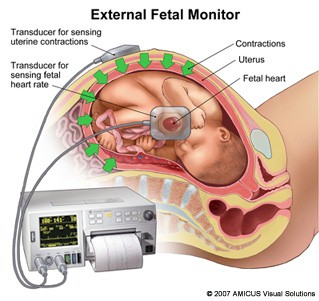
-During contraction, the FHR (fetal heart rate) slows to 10-20 beats/min. & return to normal (140-160/min.) as the intensity of contraction decreases.
Download the App: Android App
For more Lectures, please visit-
YouTube Channel – NursingLecture
Facebook – Facebook Page