Glomerulonephritis is a group of diseases that injure the part of the kidney that filters blood.
1) Acute Glomerulonephritis:-
Is know to follow acute infection & characteristically presents as acute nephritic syndrome. Acute post-streptococcal glomerulonephritis is the most common form of glomerulonephritis in children 6-16 yrs of age.
Grossly– The kidneys are symmetrically enlarged weighing one or 1½ – twice the normal weight. The cut section shows petechial hemorrhage (small spot under the skin due to the effusion of blood) giving the appearance of the “flea-bitten kidney”(unpleasant appearance).
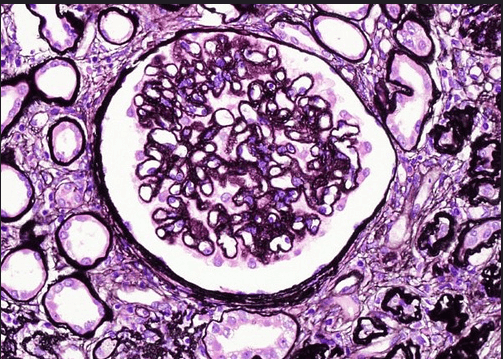
Microscopically-Glomeruli is affected by diffusely. They are enlarged & hypercellular, due to the proliferation of tuft (bunch or collection) mesangial, epithelial or endothelial cells. Tubules may show swelling, there may be interstitial edema & leucocytic infiltration.
2) Rapidly Progressive Glomerulonephritis:-
It presents with acute renal failure in a few weeks or months.
Grossly– The kidney is usually enlarged & pale with the smooth outer surface. Cut surface shows pale cortex & congested medulla.
Microscopically-Crescents(curved sickle shape) are seen inside the Bowman’s capsule.
Glomerular tufts frequency contain fibrin thrombi.
3) Chronic Glomerulonephritis:-
The end-stage kidney is the final stage of glomerular disease.
Grossly– The kidneys are usually small & contracted, weighing as low as 50 gm each. The capsule is adherent to the cortex & the cortical surface is generally diffusely granular.
Microscopically– Glomeruli are reduced in no. & show completely tuft appearing as eosinophilic masses.
– Many tubules completely disappear, may be atrophy of the tubules close to scarred glomeruli.
– There is fine delicate fibrosis of the interstitial tissue & varying no. of chronic inflammatory cells.