It is defined as an acute inflammation of the lung parenchyma distal to the terminal bronchioles.
Pathogenesis:- Microorganism gain entry into lungs by-
- Inhalation of microbes present in the air.
- Aspiration of the organism from nasopharynx or oropharynx.
- Haematogenous spread from the distant spread.
- Direct spread from the adjoining site of infection.
Classification:-
A) Bacterial Pneumonia
- Lobar Pneumonia
- Broncho Pneumonia(Lobular)
B) Viral or mycoplasmic Pneumonia
C) Pneumonia from other types-
- Pneumocystis Carinii Pneumonia
- Legionella Pneumonia
- Aspiration Pneumonia
- Hydrostatic
- Lipid
A) Bacterial Pneumonia
It is the most common cause of pneumonia, consolidation of 1 or both the lungs can be seen. In these 2 types are-
I. Lobar:-
It is an acute bacterial infection of a part of a lobe, the entire lobe, or even 2 lobes of 1 or both the lungs.
Etiology-
Microbial agent cause lobar pneumonia as-
- Pneumococcal pneumonia
- Staphylococcal pneumonia
- Streptococcal pneumonia
- Gram negative bacteria such as Haemophilus influenza, klebsiella, pseudomonas etc.
Morphological features:-
Lobar pneumonia has 4 pathologic phases, as-
1. Stage of congestion(Initial Phase)-
It represents an early inflammatory response to bacterial infection lasts for 1-2 days.
Grossly-
Affected lobe is enlarged, heavy dark red or congested.
Histologically-
Dilatation & congestion of capillaries. pale eosinophilic edema fluid in the air spaces. A few red cells & neutrophils in intra alveolar fluid.
2. Red Hepatisation (Early consolidation)-
It lasts for 2-4 days. Term hepatization refers to the liver like the consistency of the affected lobe.
Grossly-
Affected lobe is red, firm or consolidated. Involve lobe is airless, red pink, dry, granular has liver-like consistency.
Histologically-
The edema fluid is replaced by strands of fibrin. There is marked cellular exudate of neutrophils & alveolar septa are less prominent.
3. Grey Hepatisation & late consolidation-
It lasts for 4-8 days.
Grossly-
The affected lobe is firm or heavy. The cut surface is dry, granular, grey in appearance with liver-like consistency. Change in color from red to grey begin at the hilum & spread towards the periphery.
Histologically-
Fibrin strands are dense or numerous. Neutrophils are reduced & macrophages begin to appear. Cellular exudate is separated from the septal wall by thin clear space.
4. Resolution-
It begins by 8-9day & is completed in 1-3 weeks.
Grossly-
Solid fibrinous constituent is liquefied by enzymatic action & restore normal aeration in the affected lobe. The process of softening begins centrally & spread to the periphery and dirty brown, creamy yellow fluid can be expressed.
Histologically-
Macrophages are predominant cells. Fragmented strands of fibrin seen in alveolar spaces.Progressive removal of fluid content from air spaces by expectoration, or by lymphatics resulting in the restoration of normal lungs parenchyma with aeration.
II. Bronchopneumonia [Lobular]:-
Is infection of the terminal bronchioles that extends into the surrounding alveoli resulting in patchy consolidation of the lungs.
Etiology-
Common organism responsible are staphylococci, streptococci, pneumococci, Klebsiella, Haemophilus influenza, gram –ve like pseudomonas etc..
Morphological features-
Grossly-
Bronchopneumonia is identified by patchy areas of red or grey consolidation affecting one or more lobe, frequently bilaterally, involving lower zone of lung patchy lesions are dry, granular, firm red or grey in color, slightly elevated over the surface & centered around bronchiole.
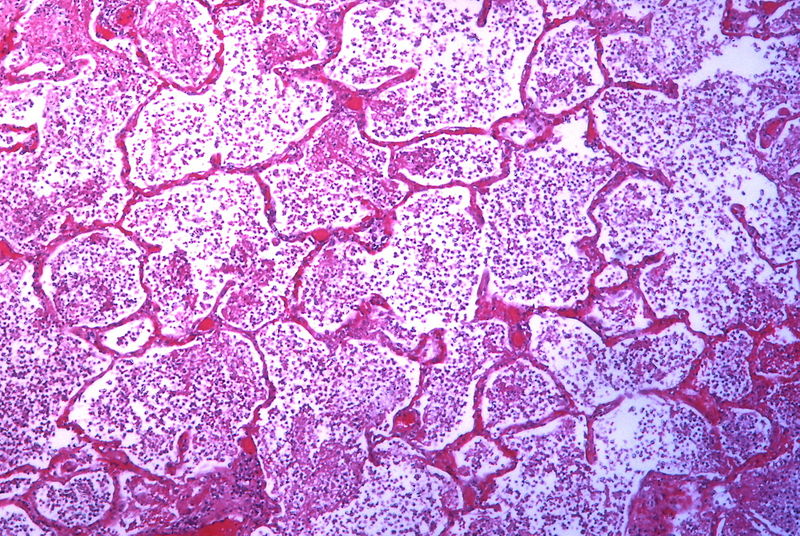
Histologically-
Neutrophils in the periphery of bronchiolar alveoli. Thickening of alveolar septa by congested capillaries or less involved alveoli contain edema fluid.
(B) Viral and Mycoplasmal Pneumonia
It is characterized by patchy inflammatory changes confined to interstitial tissues of the lung without alveolar exudates.
Etiology-
Caused most commonly by respiratory syncytial viruses others are mycoplasma, influenza, adenoviruses, rhinoviruses, CMV cytomegalovirus.
Morphological features:-
Pathologic changes are similar in all cases.
Grossly-
The involvement may be patchy to massive & consolidation of one or both of lungs. Lungs are heavy, or congested.
Histologically-
There is interstitial nature of inflammatory reaction feature are as-
- Interstitial inflammation– There is thickening of alveolar walls due to congestion mononuclear inflammatory infiltrate comprised by lymphocytes, macrophages, or plasma cells.
- Necrotizing bronchiolitis – characterized by necrosis of the bronchiolar epithelium.
- Reactive changes – the lining of epithelial cells of bronchioles & alveoli proliferate in the presence of virus & form multinucleate giant cells.
- Alveolar changes– In severe cases, alveolar lumina may contain edema fluid, inflammatory exudates.
(C) Pneumonia from other types
Some types caused by infective agents(such as pneumocystis carinii pneumonia & Legionella pneumonia ) & non infective like aspiration pneumonia, hypostatic pneumonia & lipid pneumonia.
1. Pneumocystis Carinii
-A protozoan spread in the environment caused by inhalation of an organism in neonates or immunosuppressed people.
2. Legionella pneumonia
– It is an epidemic illness caused by gram-negative bacilli. It is spread by contaminated drinking water.
3. Aspiration pneumonia
– It results from inhalation of different agent substances include food, gastric content, infected material from the oral cavity.
4. Hypostatic pneumonia
– In the edema fluid & secretions collected in the lungs(dependent part), in a bedridden patient.
5. Lipid pneumonia
– This is caused by aspiration of oily materials or tissues breakdown following obstruction to the airway.