Mycobacterium tuberculosis causes TB in the lungs or other tissues of the human body. Robert Koch first discovered the organism in 1882. The organism is strict aerobe, so survive in tissues with high oxygen like an apex of the lung.
Mode of transmission
It can be transmitted by-
- Inhalation of organism present in cough
- Inoculation into the skin
- Ingestion of bacilli from the milk of infected cow.
- Transplacental via infected mother to foetus.
Evolution
- Tubercle bacilli as enters into the pulmonary capillary, neutrophils activated by the initial response but rapidly destroyed by an organism.
- Infiltration by macrophages after 12hrs, because bacilli coated with serum complement factors C2a or C3b & attract the macrophages.
- Phagocytosis occurs, bacilli become die but further proliferate.
- Body’s immune response activates the T or B cells. Activated CD4+T cell develops cell-mediated hypersensitivity reaction, B cell forms antibodies.
- Within 2-3 days macrophages change structurally like an epithelial hence called epithelioid cell due to immune response-as cytoplasm become pale or eosinophilic & nuclei become elongated.
- Epithelioid form tight clusters (granuloma) or release cytokines IF, IL, TNF etc. In response to activated CD4+T cells.
- Some of the macrophages form a multinucleated giant cell, by fusion of cell, especially of langhan’s type in which nuclei arranged in peripherally like a horseshoe or clustered at 2 opposite pole, or maybe foreign body type- nuclei arranged centrally.
- Around the epithelioid cells or giant cell, there is a zone of lymphocyte, plasma cell or fibroblast. the lesion called hard tubercle.
- Within 10-14 days, central mass begins to undergo caseation necrosis (cheesy appearance) & form soft tubercle.
Types
Depending upon the tissues response or age it is of 2 main types:
A) Primary TB
-The individual who has not been previously infected, also known as Ghon’s complex or childhood TB.
–It is the lesions produced in the tissues of the portal of entry with foci in draining lymphatic vessel & lymph node. Most commonly involved are tissues of lungs or hilar lymph node. Incidence is commonly seen in immune compromised persons.
Ghon’s complex in lungs consist of 3 component-
- Pulmonary component:- Lesion is 1-2 c.m. solitary area located peripherally in the upper part of the lower lobe.
- Lymphatic vessel component:– Draining lung lesion contain phagocyte, may develop beaded, miliary tubercles along the path of a hilar lymph node.
- Lymph node component:– Affected lymph node shows caseation necrosis. It consists of an enlarged hilar & tracheobronchial lymph node.
Fate of primary TB
- The lesion does not progress but heal by fibrosis & undergo calcification.
- In some primary focus continue to grow caseous material disseminated through bronchi to other parts of the lung is progressive primary TB.
- Bacilli enter the circulation by erosion in a blood vessel & spread to various tissues, called primary miliary TB. The lesion is seen in the liver spleen, kidney, bone etc.
- In some lowered resistance host, healed lesion of primary TB get reactivated cause secondary progressive TB.
B) Secondary TB
The infection of an individual who has been previously infected is called post-primary TB, reinfection or chronic TB. The lesion in secondary TB begins as 1-2 c.m. apical area of consolidation, which may occur by the haematogenous spread of infection from primary complex to apex, where high O2 tension favoured the growth of bacilli.
Fate of secondary TB
- The lesion may heal fibrous scarring or calcification.
- Lesions may coalesce together & produce progressive secondary PTB with extrapulmonary involvement like-
- Fibrocaseous TB:- Area of tuberculous pneumonia undergo central caseation necrosis may break into a bronchus from a cavity (cavitary open TB ) or remain soft caseous lesion without drainage into bronchus produce non-cavitary lesion.
- Tuberculous Caseous Pneumonia:- Caseous material may spread to the rest of the lung produces caseous pneumonia.
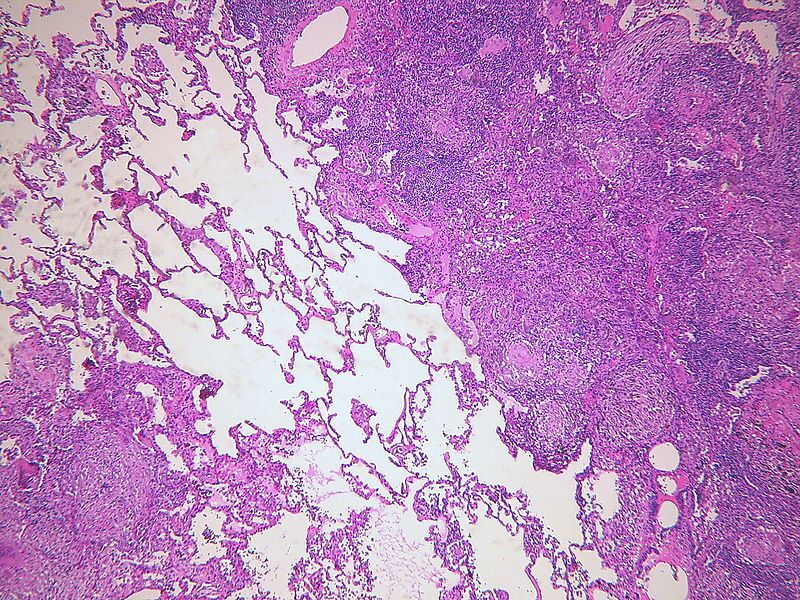
- Miliary TB:- Due to the spread of infection through lymphohematogenous route to form multiple tiny lesion called military TB. Expand to involve large area, lesion resembles millet seeds. It can confine to lungs or extrapulmonary spread.