PEPTIC ULCERS

Peptic ulcer disease (PUD) is a break in the inner lining of the stomach, the first part of the small intestine or sometimes the lower esophagus.
MORPHOLOGICAL FEATURES
1) Acute Peptic Ulcer:-
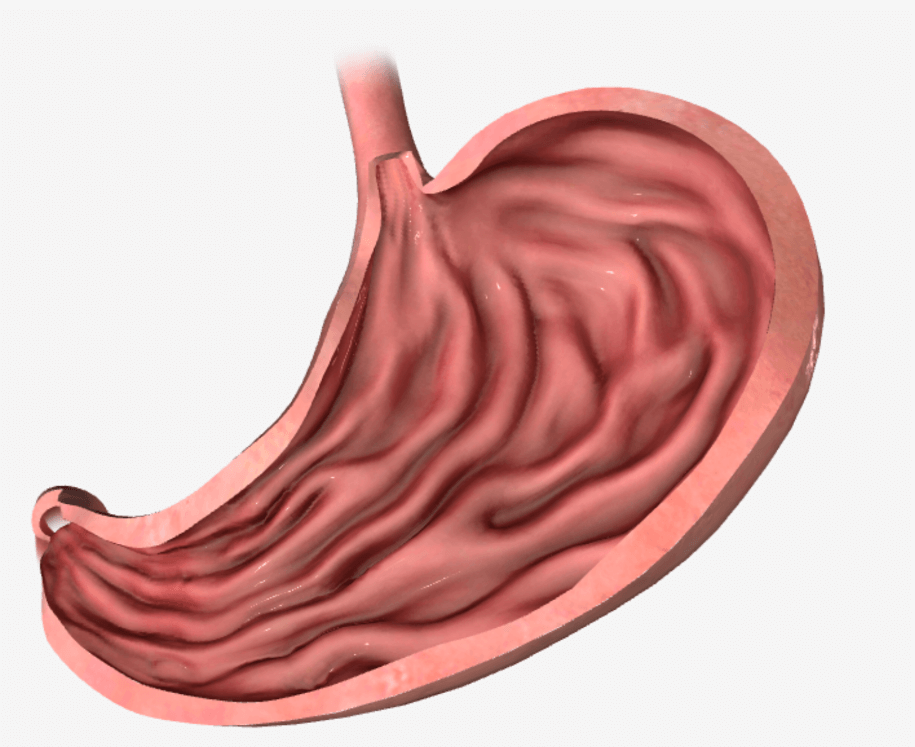
Grossly- Acute ulcers are multiple. They are more common anywhere in the stomach decreasing frequently in the first part of the duodenum. They may be oval or circular in shape.
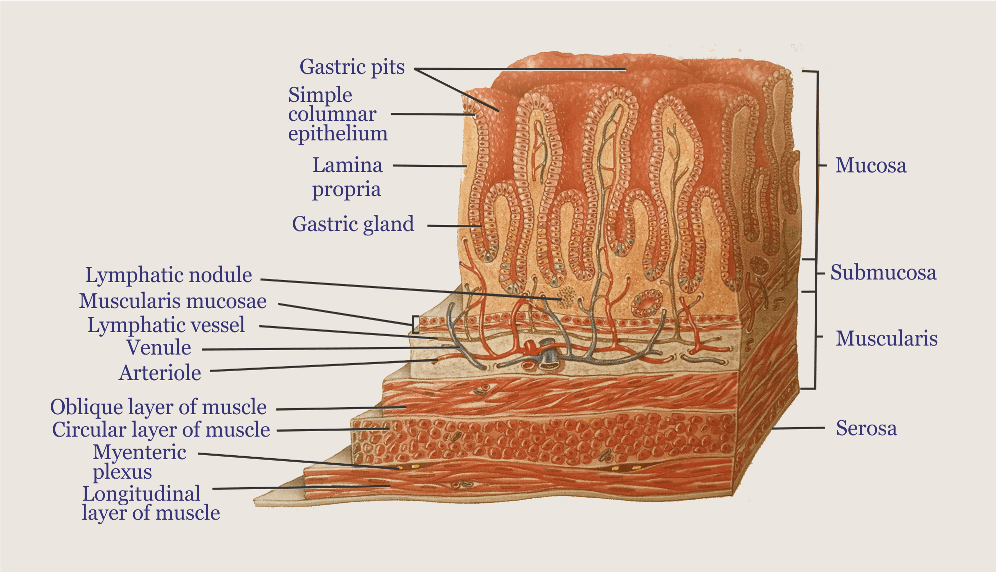
Microscopically- They are shallow, do not invade the muscular layer. Margin & base show inflammatory reactions. These commonly heal by re-epithelialization without leaving any scars.
2) Chronic Peptic Ulcer:-
Grossly- Grossly gastric & duodenal ulcers are similar. Ulcers are commonly solitary, small (1-1.25cm in diameter), round to oval & characteristically ‘punched out’. Ulcers may vary in depth from being superficial to deep ulcers (mucosa to muscular layer).
-Most are benign <1% can turn into a malignant form which is larger, bowl shaped with elevated mucosa at margins. Gastric ulcer is found along the lesser curvature in the region of pyloric antrum & duodenal ulcers are found in the first part of the duodenum (post-pyloric).
Microscopically- Have 4 histological zones, from within outside:-
• Necrotic Zone:- Lies in the floor of the ulcer & composed of fibrous exudates containing necrotic debris.
• Superficial exudative zone:- lies underneath of necrotic zone. Tissue elements show coagulative necrosis giving eosinophilic, smudgy (dirty mark) appearance.
• Granulation tissue Zone:- Merging into a necrotic zone, composed of nonspecific inflammatory infiltrate.
• Zone of cicatrization:- It is merging into a thick layer of granulation tissue composed of the dense fibro collagenic scar. Thrombosed arteries may cross the ulcer which on erosion may result in hemorrhage.